Evaluating a Bundled Protocol to Reduce Aspiration Pneumonia in Critically Ill Tube-Fed Patients
DOI:
https://doi.org/10.54133/ajms.v10i2.2872Keywords:
Aspiration pneumonia, Critical care , Bundle protocol , Enteral feeding , Nasogastric tube , Quality improvementAbstract
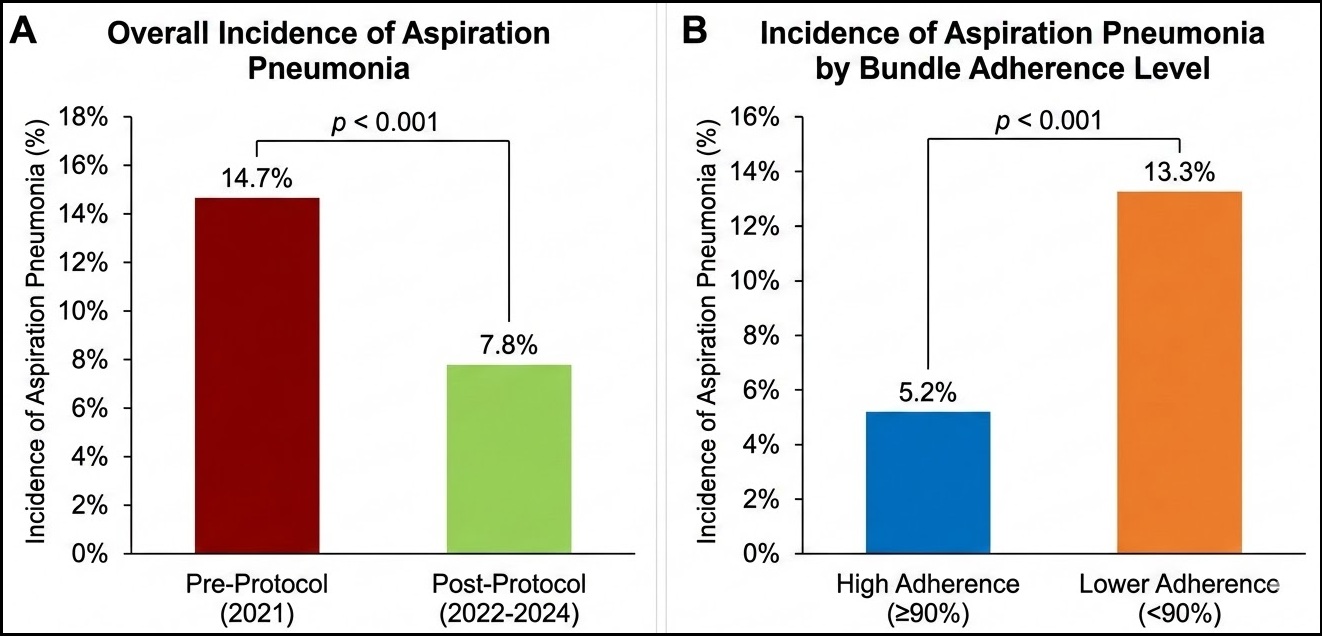
Background: Patients who are severely ill and are fed through a nasal tube mostly suffer from aspiration pneumonia. Objective: To evaluate the degree to which an exploratory, evidence-based, and multifaceted method lowered the aspiration pneumonia in critically ill tube-fed patients. Methods: A historical observation group study was carried out by the Critical Care Unit at a tertiary care hospital. For the period of January to December 2021, a control group consisting of 415 individuals got usual care. This group was compared to an experimental group consisting of 2,120 individuals who received additional help for the period of January 2022 to December 2024. As part of the combining method, 30–50 mL of water were flushed after each enteral dose, drugs were given as normal (crushing, decreasing, and flushing between doses), and overnight fasting was strictly limited to six hours. The main effect was incidents of aspiration pneumonia. Results: The intended surgery reduced aspiration pneumonia from 14.7% to 7.8%. After controlling for other factors, the method reduced aspiration pneumonia by 52% (OR=0.48, 95% CI=0.35–0.66). Bundling adherence (≥90%) was linked to decreased incidence (5.2% vs. 13.3% for poor adherence). Reduced median ICU stay (7.0 days vs. 9.0 days) and 22% fewer antibiotic days were noteworthy advantages. Conclusions: Placing forward a cohesive aspiration prevention plan approach led to fewer incidents of aspiration pneumonia and favorable secondary clinical outcomes in critically ill patients who received nutrition by tube. In critical care, this practical procedure assists in making enteral nutrition safer and superior.
Downloads
References
Alkhawaja S, Martin C, Butler RJ, Gwadry-Sridhar F. Post-pyloric versus gastric tube feeding for preventing pneumonia and improving nutritional outcomes in critically ill adults. Cochrane Database Syst Rev. 2015;(8):CD008875. doi: 10.1002/14651858.CD008875.pub2. DOI: https://doi.org/10.1002/14651858.CD008875.pub2
Jiyong J, Tiancha H, Huiqin W, Jingfen J. Effect of gastric versus post-pyloric feeding on the incidence of pneumonia in critically ill patients: observations from traditional and Bayesian random-effects meta-analysis. Clin Nutr. 2013;32(1):8-15. doi: 10.1016/j.clnu.2012.07.002. DOI: https://doi.org/10.1016/j.clnu.2012.07.002
Deane AM, Guy S, Koopmans R, Page K, Regli A. Routine monitoring of gastric residual volume not recommended. Intensive Care Med. 2023;49(1):81-84. doi: 10.1007/s00134-022-06938-6.
Poulard F, Dimet J, Martin-Lefevre L, Bontemps F, Fiancette M, Lemiale V, et al. Impact of not measuring residual gastric volume in mechanically ventilated patients receiving early enteral feeding: a prospective before-after study. J Parenter Enteral Nutr. 2010;34(2):125-130. doi: 10.1177/0148607109344745. DOI: https://doi.org/10.1177/0148607109344745
McClave SA, Gualdoni J, Nagengast A, Dietsche C, Gott A, Guenter P, et al. Gastric feeding tubes in the critically ill patient. Gastroenterol Clin North Am. 2022;51(4):703-721. doi: 10.1016/j.gtc.2022.07.004. DOI: https://doi.org/10.1016/j.gtc.2022.07.004
Blaser AR, Deane AM, Fruhwald S, van Zanten ARH. Gastrointestinal function in the critically ill: a systematic scoping review and research agenda proposed by the Section of Metabolism, Endocrinology and Nutrition of the European Society of Intensive Care Medicine. Crit Care. 2020;24(1):224. doi: 10.1186/s13054-020-02937-7. DOI: https://doi.org/10.1186/s13054-020-02889-4
Boullata JI, Carrera AL, Harvey L, Hudson L, Mays A, McGinnis C, et al. ASPEN safe practices for enteral nutrition therapy. J Parenter Enteral Nutr. 2017;41(1):15-103. doi: 10.1177/0148607116673053. DOI: https://doi.org/10.1177/0148607116673053
Reignier J, Boisramé-Helms J, Brisard L, Lascarrou JB, Ait Hssain A, Anguel N, et al. Enteral versus parenteral early nutrition in ventilated adults with shock: a randomised, controlled, multicentre, open-label, parallel-group study (NUTRIREA-2). Lancet. 2018;391(10116):133-143. doi: 10.1016/S0140-6736(17)32146-3. DOI: https://doi.org/10.1016/S0140-6736(17)32146-3
Klompas M, Branson R, Cawcutt K, Crist M, Eichenwald EC, Greene LR, et al. Strategies to prevent ventilator-associated pneumonia, ventilator-associated events, and nonventilator hospital-acquired pneumonia in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol. 2022;43(6):687-713. doi: 10.1017/ice.2022.88. DOI: https://doi.org/10.1017/ice.2022.88
O'Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011;52(9):e162-e193. doi: 10.1093/cid/cir257. DOI: https://doi.org/10.1093/cid/cir257
Metheny NA, Frantz RA. Head-of-bed elevation in critically ill patients: A review. Crit Care Nurse. 2013;33(4):53-66. doi: 10.4037/ccn2013572. DOI: https://doi.org/10.4037/ccn2013456
Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355(26):2725-2732. doi: 10.1056/NEJMoa061115. DOI: https://doi.org/10.1056/NEJMoa061115
Resar R, Pronovost P, Haraden C, Simmonds T, Rainey T, Nolan T. Using a bundle approach to improve ventilator care processes and reduce ventilator-associated pneumonia. Jt Comm J Qual Patient Saf. 2005;31(5):243-248. doi: 10.1016/s1553-7250(05)31031-2. DOI: https://doi.org/10.1016/S1553-7250(05)31031-2
Metheny NA, Davis-Jackson J, Stewart BJ. Effectiveness of an aspiration risk-reduction protocol. Nurs Res. 2010;59(1):18-25. doi: 10.1097/NNR.0b013e3181c3ba05. DOI: https://doi.org/10.1097/NNR.0b013e3181c3ba05
McClave SA, DeMeo MT, DeLegge MH, DiSario JA, Heyland DK, Maloney JP, et al. North American Summit on Aspiration in the Critically Ill Patient: consensus statement. J Parenter Enteral Nutr. 2002;26(6 Suppl):S80-S85. doi: 10.1177/014860710202600612. DOI: https://doi.org/10.1177/014860710202600613
Blot SI, Poelaert J, Kollef M. How to avoid microaspiration? A key element for the prevention of ventilator-associated pneumonia in intubated patients. BMC Anesthesiol. 2014;14:92. doi: 10.1186/1471-2253-14-92. DOI: https://doi.org/10.1186/1471-2334-14-119
Davies AR, Morrison SS, Bailey MJ, Bellomo R, Cooper DJ, Doig GS, et al. A multicenter, randomized controlled trial comparing early nasojejunal with nasogastric nutrition in critical illness. Crit Care Med. 2012;40(8):2342-2348. doi: 10.1097/CCM.0b013e318255d87e. DOI: https://doi.org/10.1097/CCM.0b013e318255d87e
Mandell LA, Niederman MS. Aspiration pneumonia. N Engl J Med. 2019;380(7):651-663. doi: 10.1056/NEJMra1714562. DOI: https://doi.org/10.1056/NEJMra1714562
Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013;39(2):165-228. doi: 10.1007/s00134-012-2769-8. DOI: https://doi.org/10.1007/s00134-012-2769-8
Metheny NA, Mills AC, Stewart BJ, Oliver D, Clouse RE. A comprehensive algorithm to detect aspiration in enterally fed critically ill patients. Am J Crit Care. 2021;30(5):371-379. doi: 10.4037/ajcc2021789.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Al-Rafidain Journal of Medical Sciences ( ISSN 2789-3219 )

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Published by Al-Rafidain University College. This is an open access journal issued under the CC BY-NC-SA 4.0 license (https://creativecommons.org/licenses/by-nc-sa/4.0/).